
Syndesmosis Injury Rehab
Meet James
James is a 25-year-old competitive AFL player who sustained a left knee hyperextension injury during an AFL game. Our match-day physiotherapist assessed him on the sideline and was concerned about both an ACL rupture and a possible fracture. James was admitted to Royal Prince Alfred Hospital for assessment and discharged to our care.
Following his examination, our physiotherapist ordered an X-ray which identified an acute Segond fracture at the lateral tibial plateau. This finding, along with the mechanism of injury prompted a referral to his GP who was able to order a bulk billed MRI. Unfortunately the MRI confirmed a complete ACL rupture. A referral to an orthopaedic knee surgeon was arranged. Following the orthopaedic assessment surgery was scheduled in a month later, an ACL reconstruction using a hamstring autograft combined with a lateral tenodesis.

The good news: At week 38, James has been training with the men’s AFL squad, stopping before contact. Strength and power numbers are approaching symmetry.
Understanding the injury
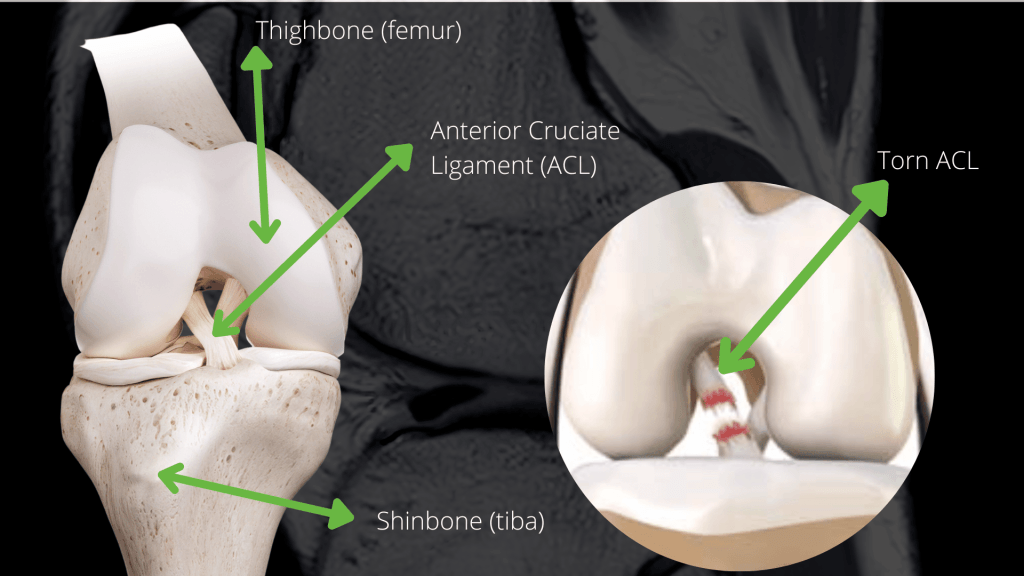
The ACL is the primary restraint against the tibia (shin bone) sliding forward and rotating on the femur (thigh bone). In field sports like AFL, ACL injuries can occur through several mechanisms including a sudden change of direction, rapid deceleration, direct contact to the knee, or a hyperextension under load. No single mechanism is universal. (Grassi et al., 2021; Losciale et al., 2022)
The Segond fracture, a small bony chip at the outer edge of the shin bone, is an important finding because it indicates significant rotational instability and disruption of the ligaments on the outer side of the knee. It was this finding on X-ray along with the mechanism described and his clinical presentation that prompted the MRI, confirming the full picture. Without the physio examination and then X-ray, the extent of the injury may have been missed at that initial presentation. (Flores et al., 2021)
Without reconstruction, an ACL-deficient knee in a high-demand athlete carries a meaningful risk of ongoing instability and damage to the meniscus and cartilage over time. (Grassi et al., 2021)
Why a lateral tenodesis was added
A standard ACL reconstruction replaces the torn ligament with a new graft, in James’s case, using his own hamstring tendon. However, given the rotational instability identified by the Segond fracture, his surgeon also performed a lateral tenodesis.
A lateral tenodesis is an additional procedure that reinforces the outer side of the knee using a small strip of the iliotibial band, anchored to bone. Think of it as adding a secondary restraint against the rotational forces that put grafts at greatest risk. In young athletes returning to pivoting sports, research suggests this addition may reduce graft re-rupture rates by up to 50% compared to ACL reconstruction alone. (Getgood et al., 2020; Inderhaug et al., 2022)
It does not significantly change the rehabilitation timeline, but it does address a specific vulnerability that the imaging identified in James’s case

The role of prehabilitation
Prehabilitation is physio rehab completed before surgery. It is one of the most impactful parts of ACL care, but also one of the most commonly skipped. James began prehab immediately after injury, before his surgery date was even confirmed.
The goals were straightforward: reduce swelling, restore as much knee range of motion as possible, reactivate the quad and hamstring muscles, and maintain lower limb strength. Patients who arrive at surgery with better strength and muscle control tend to recover faster and reach key milestones earlier in their post-operative rehabilitation. (Calatayud et al., 2022; Albano et al., 2021)
Arriving at the operating table in better physical condition is one of the few things a patient can directly control before surgery and the evidence consistently supports doing so.

The rehabilitation journey
ACL rehabilitation typically spans 12-18 months from surgery to return to sport. The physiotherapist’s role shifts at every phase, from swelling control and gait retraining in the early weeks, through targeted strength rebuilding and neuromuscular retraining in the middle phase, to coaching and cuing a demanding gym and plyometric program as functional demands and return to sport approaches. Manual therapy, soft tissue work, load management abd specific coaching sit alongside the gym program throughout as required. The surgeon’s protocol guides the overall framework, with physio tailoring every session to what James’s knee was showing that day.
Phase 1 | Weeks 0-2
Swelling control, quad activation, gentle range of motion targeting full extension, and gait retraining with crutches. The graft is most vulnerable here — early care is about protecting it while beginning to move.
Phase 2 | Weeks 2-6
Progressing off crutches, achieving full range of motion, and beginning closed-chain strengthening: step-ups, wall squats, leg press, and hamstring work. Proprioception and cardiovascular fitness introduced via bike, elliptical, and aquatic therapy.
Phase 3 | Weeks 6-12
More dynamic gym loading across all lower limb exercises. Open-chain knee extension is still avoided — the graft is at its biological weakest in this phase. Running in a straight line may commence from 12 weeks when strength and range of motion criteria are met.

Phase 4 | Weeks 12-20
Jumping and hopping introduced with emphasis on landing technique. Agility work begins: lateral running, shuttle drills, and sport-specific movement. This is where the program begins to look like AFL preparation.
Phase 5 | Weeks 20+: Return to training
Strength continued to build and in clinic structured contact preparation began: partner push, jostling, swissball tackles, contested marks. Progressive reintegration with the men’s AFL squad for skills and drills, however not participating in full contact. Progression is criteria-based. James advances when the data supports it. (Grindem et al., 2020; Kyritsis et al., 2022)

Measuring progress: from early testing to week 38
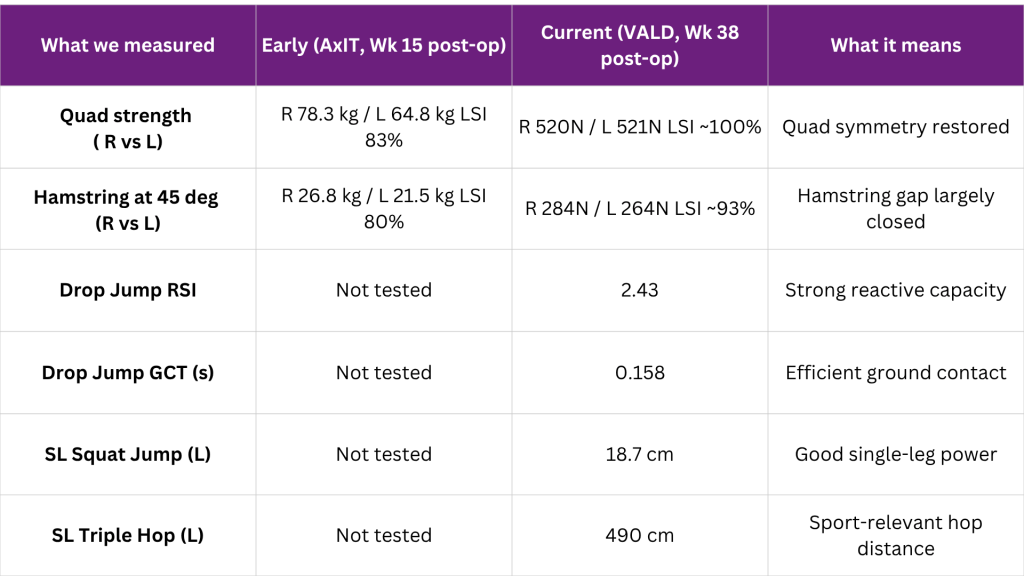
James’s strength has been tracked across his rehabilitation using two platforms. Early strength data (week 15) was captured using AxIT dynamometry. Current data (week 38) uses VALD dynamometry and ForceDecks, a system we recently switched to. Both measure peak force output and limb symmetry, though the units differ between platforms. The amount of improvement, and the scale of it is what matters here. We also measure compared to the non-operative leg using a measure known as LSI (Leg Symmetry Index)
Note: AxIT and VALD use different setups and units. LSI comparisons (comparing to the opposite leg) across platforms reflect the direction of change rather than direct equivalents. Quad LSI improved from 83% in January to near-symmetry in June. Hamstring LSI at 45 degrees improved from 80% to approximately 93%. Drop jump and hop data were not collected at week 15 and represent current capacity only.
Criteria for return to sport
Returning to AFL too early is one of the most preventable causes of ACL re-rupture. Research shows that athletes who return to pivoting sport before nine months post-surgery are up to four times more likely to sustain a graft re-rupture than those who wait. (Grindem et al., 2020; Kyritsis et al., 2022) Time alone, however, is not the answer. Athletes need to meet objective criteria and be gradually exposed to their environment to return safely.
Where to from here for James
James is at a genuinely exciting point in his rehabilitation. At week 38, his quadriceps are essentially symmetrical and his hamstring LSI has closed from 80% at week 15 to 93% now. His drop jump RSI of 2.43 reflects real reactive power, the kind his sport demands. He has been integrating with the men’s AFL squad in contact preparation sessions and the next step is unrestricted full-contact drills.
The main remaining objective benchmark is the hop test battery — specifically the SL triple hop, where his left limb is currently at 86% LSI against the right. This reflects an ongoing asymmetry in single-leg power output that the program is actively targeting. It is not a barrier to continued training, it is the next milestone.
The plan for James over the coming weeks:
- Continue gym loading, targeting hamstring strength and hop test symmetry
- Progress through full squad contact sessions, working towards unrestricted match play
- Repeat VALD and hop testing to confirm all criteria are met before match clearance
- Ski trip in August as a functional confidence benchmark outside of AFL
- Final return-to-sport criteria sign-off in collaboration with his orthopaedic surgeon
James came in with a clear goal: return to AFL. Everything between day one post-op and now has been in service of that goal. The data says he is close. When he runs out for his first full-contact game, it won’t be a leap of faith, it will be a decision backed by a clear set of numbers saying the knee is ready.

If you or someone you care for has an injury, a flare up, requires some rehabilitation or experiences an increase in pain, give the clinic a call on 9713 2455 or book online.