
Syndesmosis Injury Rehab
Meet Steven
Steven is a 27-year-old recreational soccer player. He trains twice a week, playing weekend games, and fitting in swimming and running when he can.
His injury happened suddenly. He was performing a box jump when the box tipped, and he landed with his foot twisted outward. He heard a loud crack and felt the ankle give way. He presented to Total Body Physio in a CAM boot, unable to weight-bear, with significant swelling and bruising throughout the ankle.

What We Found
On assessment, Steven presented with:
- Global bruising and significant swelling
- Inability to perform a single leg calf raise
- Tenderness over the syndesmosis, deltoid ligament, and distal fibula
- Significantly restricted ankle dorsiflexion
- Positive syndesmosis provocation testing (external rotation stress)
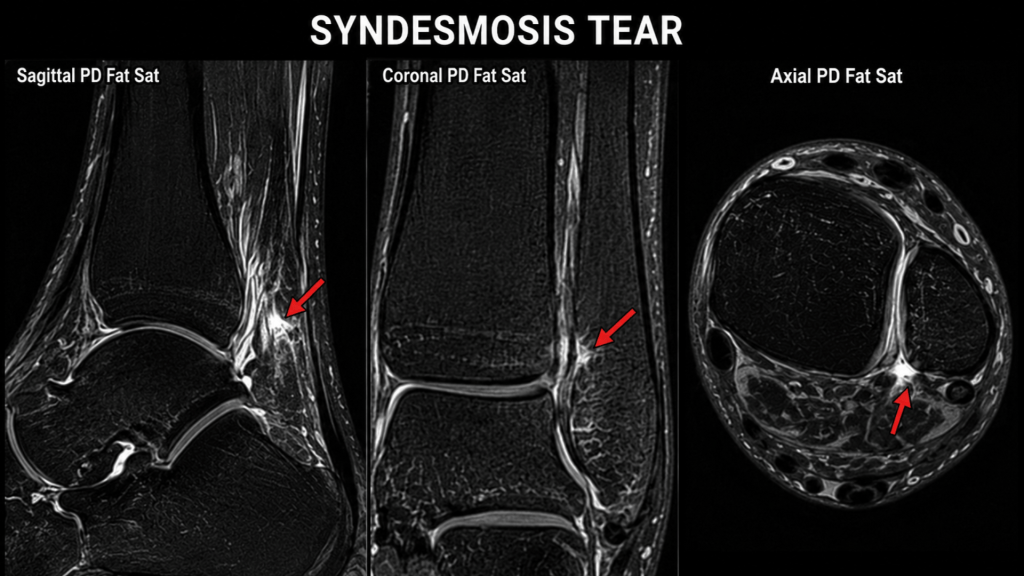
With this presentation we sent him for an x-ray that identified a fibular fracture. However, given the strong clinical picture of syndesmotic injury, we arranged an MRI. This confirmed a displaced Weber B fibular fracture at the level of the syndesmosis, a complete rupture of the anterior syndesmosis, a partial-thickness ATFL tear, and a low-grade deltoid ligament sprain.

Why Did This Happen?
The syndesmosis is the fibrous joint that binds the two shin bones, the tibia and fibula together just above the ankle. It is held in place by a set of ligaments that act as a stabilising bracket, keeping the ankle stable during every step, jump, and change of direction.
When Steven landed with his foot everted and plantarflexed he tore through the anterior syndesmotic ligament and fractured the fibula. Without surgical stabilisation, the ankle joint would widen, causing cartilage damage, chronic instability and early ankle arthritis. (Kale et al., 2024)
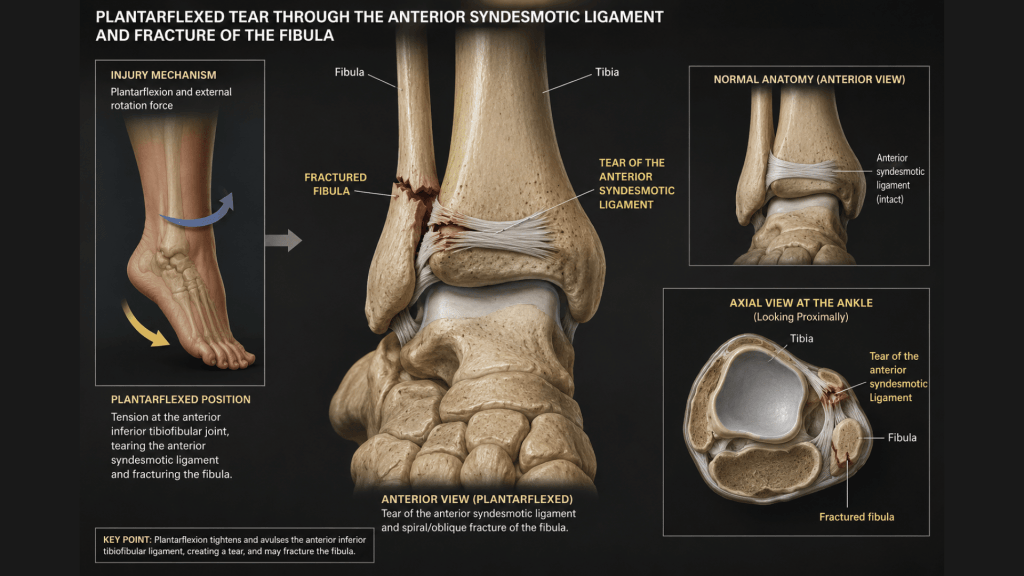
Think of the syndesmosis like a clamp holding a pipe fitting together. When it tears, the joint opens up and loading it without repair accelerates joint wear and tear.
The Surgical Decision
After liaising with his GP we referred Steven to an orthopaedic surgeon, who confirmed the diagnosis and recommended surgical stabilisation. Syndesmotic injuries with associated fibular fractures and diastasis (widening) require surgical intervention to prevent long-term instability. (Voight et al., 2024)
The operation fixed the fibular fracture with a plate and screws, and repaired the syndesmosis using a flexible suture-button device called a TightRope. Unlike a metal screw, this allows a small amount of natural movement at the joint, which is how a healthy ankle is supposed to work. It also means a second operation to remove hardware is usually not required.
Surgery is not always the answer. But for Steven, a young, active patient with a fracture and complete syndesmotic rupture, it gave him the best chance of a stable, functional ankle for the years ahead. And the evidence supported that decision.
Before Surgery: Keeping the Ankle Moving
In the weeks between injury and operation, Steven continued attending physiotherapy. The goal was not to rehabilitate the injury (that awaited surgical repair) but to maintain joint mobility, reduce swelling, and preserve as much lower limb strength as possible. Pre-operative function is an established predictor of post-operative recovery. (Carvalho et al., 2024)
This included gentle banded calf and ankle exercises, soft tissue management, ice and compression, and kinetic chain exercises to maintain hip and knee strength without loading the injured ankle.

The Post-Op Rehabilitation Journey
Rehabilitation was structured across four phases, each progressed based on what the ankle could handle — not just the calendar.
Phase 1: Weeks 6–16 | Building the Base
After surgery, Steven spent time in a fibreglass cast to allow the repair to set. Physio began at six weeks. With the ankle still protected in a boot, we focused on restoring movement and controlling swelling through manual therapy, gentle range-of-motion work, gait retraining exercises and ice and compression. Strengthening started carefully including banded exercises progressing to seated calf work, while carefully targeting the rest of his kinetic chain. As he progressed through this stage, he was able to commence more functional training for his calf and also commence gym exercises strengthening the rest of his lower limb. The goal was to build a solid foundation before asking anything more of the repaired joint.

Phase 2: Weeks 17–30 | Load and Run
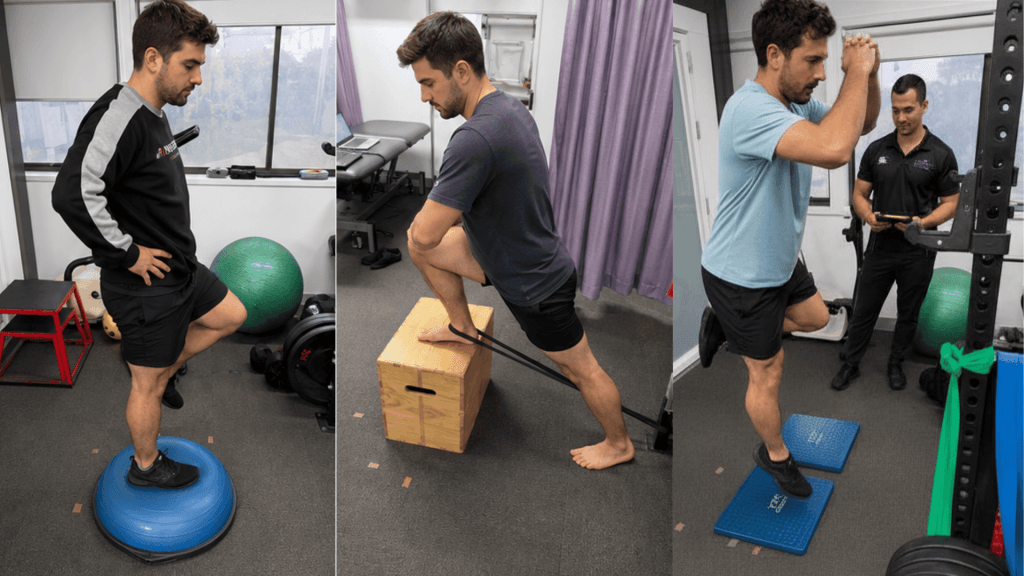
Restoring movement and calf loading was the priority. We escalated progressively from light single-leg calf work to heavy Smith machine raises, because a strong calf is what protects and stabilises the ankle long-term. Ankle dorsiflexion improved steadily and became a key target throughout this phase. Plyometrics were introduced in clinic: trampoline pogos, snapdowns, banded jogging, and jumping drills. Running began in the park with short runs first, building toward longer continuous runs. Some persistent lateral ankle discomfort emerged during high-effort direction changes, which was monitored closely and managed in collaboration with the surgeon.

Phase 3: Weeks 31–43 | Back on the Pitch
Sport-specific training ramped up: A-skips, arc runs, box and T-drills, figure-8s, and reactive change-of-direction tasks. Advanced plyometrics were included: single-leg jumps, lateral hops, skaters, and countermovement jumps. Hop testing confirmed greater than 90% limb symmetry on all tasks. This is the benchmark for safe return to cutting and pivoting sport. (Weber et al., 2024) Steven returned to half-games of soccer, progressing to full games shortly after. The FIFA warmup was integrated before every training session and game to aide with football specific training and injury prevention.
He was formally discharged with good ankle strength, near-symmetrical dorsiflexion, and full return to soccer, swimming, and running.

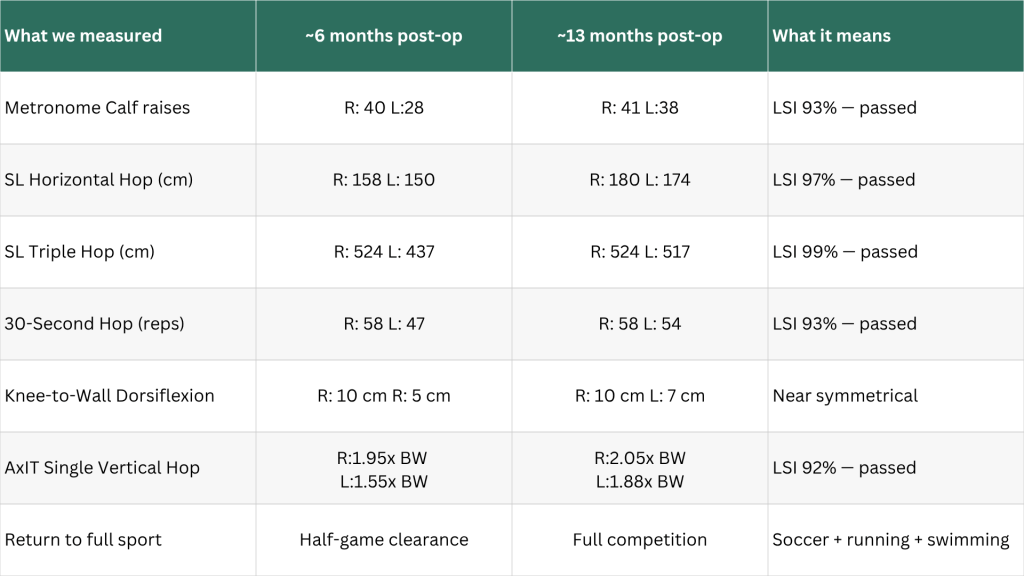
Objective Outcomes: Measuring What Matters
Rehabilitation was progressed using objective milestones, not just time. Hop testing was used to quantify limb symmetry and guide return-to-sport clearance, with a passing threshold of 90% or greater. (Weber et al., Front. Sports Act. Living, 2024)
Key Takeaways
We can happily report — Steven is back playing competitive soccer.
- Syndesmotic injuries are not simple ankle sprains. A fracture above the level of the ankle combined with ligament disruption requires imaging, careful clinical assessment, and often surgical stabilisation. Early referral matters. (Kale et al., 2024)
- Plain film X-ray can underestimate the true severity. When syndesmosis provocation testing is positive, MRI provides critical information that plain film cannot. Weber A on X-ray became Weber B on MRI in this case.
- Surgery is not always needed, but when the joint structure is compromised in an active young patient, it is often the best path to long-term stability. Post-operative return-to-sport rates following ORIF (Open Reduction and Internal Fixation) average 87%, with better outcomes tied to early, structured rehabilitation. (Carvalho et al., 2024)
- Criteria-based return to sport, not time alone, reduces reinjury risk. Steven took 13 months to return to full competition. That timeline was driven by data, not patience. Pain resolution is not a proxy for readiness.
If you or someone you care for has an injury, a flare up, requires some rehabilitation or experiences an increase in pain, give the clinic a call on 9713 2455 or book online.