
From 30 Dislocations to Back on the Netball Court
Meet Elise
Elise is a 17 year old who plays netball six times a week. She is competitive, fit, and active — but for four years, her right shoulder had been quietly getting worse.
It started with a single fall during a game. Her shoulder dislocated, she relocated it herself, and she got on with it. Then it happened again. And again. By the time she came to see us at Total Body Physio, she reports that her shoulder had dislocated or partially dislocated (subluxed) around 30 times.
She came in after her most recent dislocation hoping to avoid surgery. That was the goal. Unfortunately, it became clear that conservative management, was not going to give her the shoulder she neededgiven her sporting ambitions.

Why Was This Happening?
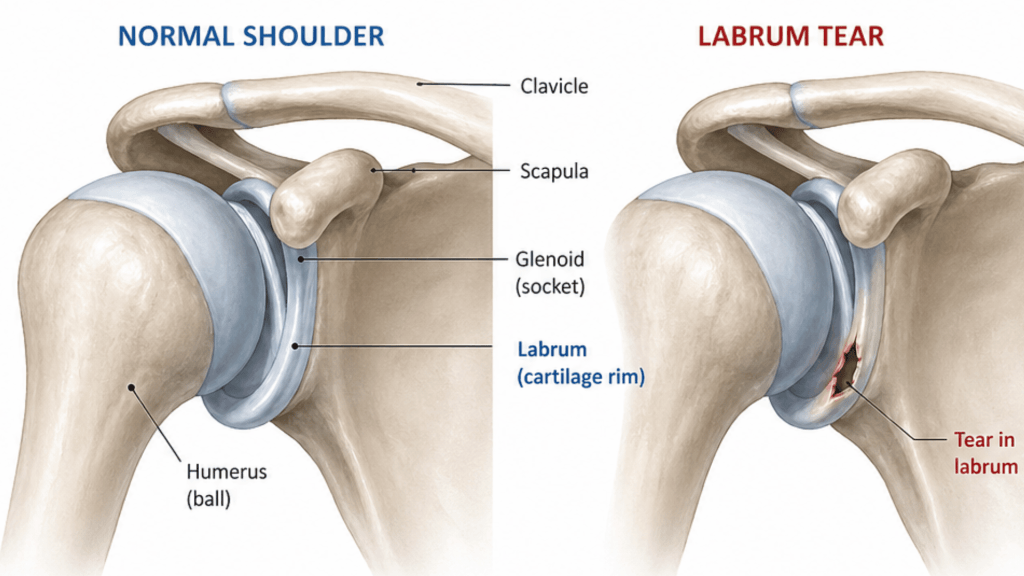
Elise’s shoulder had been dislocating because of a tear in the labrum – a ring of cartilage inside the joint that acts like a cup, keeping the ball of the upper arm seated securely in its socket. Once that ring is torn, the joint loses its structural anchor and it becomes unstable.
She also had naturally looser joints than most people (called hypermobility), which made it harder for the muscles and tissues around the shoulder to keep her stabile. The more it dislocated, the more the joint surfaces wore down, and the harder any future repair would become.
Think of it like a door hinge that keeps coming loose. Each time it slips, the screw holes get a little bigger — and eventually tightening the screws is no longer enough. Each dislocation also risks progressive bone loss on both the socket and ball of the joint, increasing the complexity of any future repair. (Willemot et al., 2022).
What We Found
On clinical assessment, Elise presented with:
- Positive apprehension test in the abducted, externally rotated position — her most provocative position
- Full active range of motion, but significant discomfort and guarding in abduction
- Weak external rotation in neutral, with measurable side-to-side asymmetry
- Positive sulcus sign indicating ligament laxity
- Scapular control deficits on the right side
- Generalised hypermobility

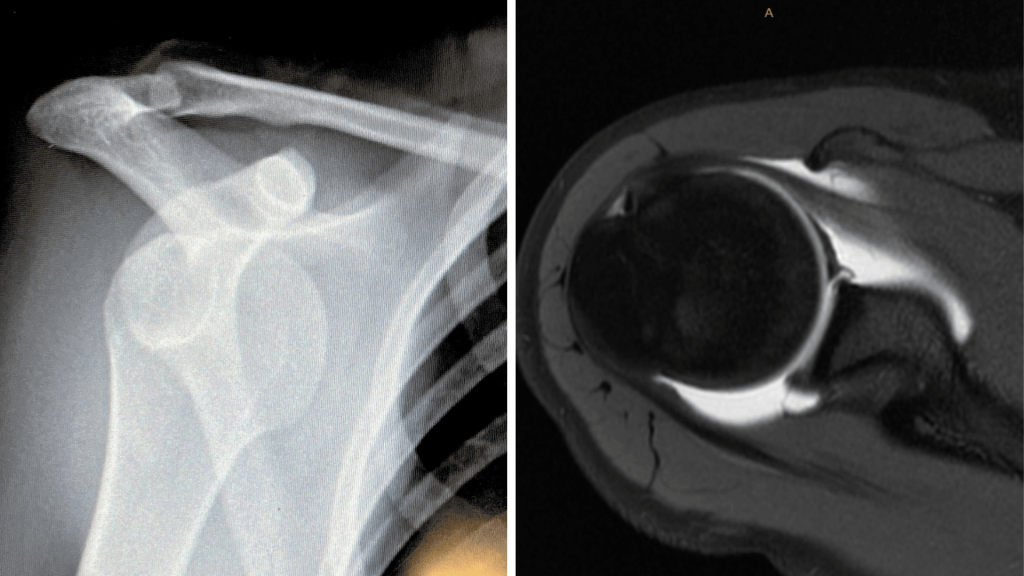
X-ray confirmed that her shoulder was relocated with no acute fracture. Given Elise’s age, activity demands, and ongoing instability, an MRI was arranged which confirmed an anteroinferior labral tear extending into the superior labrum, alongside a small Hill-Sachs defect (compression fracture on the humeral head). Current evidence supports MRI in young athletes with instability where structural findings will directly guide if surgery is warranted. (Murphy et al., 2023)
The Surgical Decision
Our Physio’s liaised with Elise’s GP, who facilitated a referral to an orthopaedic shoulder surgeon. Following review, the surgeon confirmed recurrent traumatic anterior instability on a background of hyperlaxity, with confirmed labral pathology. Both operative and non-operative options were discussed in full with Elise and her family.
In young athletes with confirmed structural instability, early arthroscopic stabilisation reduces recurrence rates to approximately 10 to 15%, compared with 50 to 90% following conservative management alone. For Elise,a 17 year old, playing high-contact sport six times a week, with multiple prior episodes and confirmed bone defects the evidence unfortunately clearly favoured surgery. (Hurley et al., 2020; Longo et al., 2020)
Surgery is never the default answer. But in Elise’s case, it gave her the best chance of a stable shoulder for the next decade of sport — and the research supported that decision.
Elise underwent right shoulder arthroscopic stabilisation. The procedure reattached the torn labrum back to the glenoid socket, tightening the joint from the inside through small keyhole incisions. She was placed in a sling for 6 weeks post-operatively.
Before Surgery: Preparing the Shoulder
In the weeks leading up to surgery, Elise’s surgeon recommended that she continue physiotherapy as pre-operative function is an established predictor of post-operative recovery (McIsaac et al., 2022). Patients who arrive at surgery stronger and more neurologically prepared tend to recover faster and more completely. (Blonna et al., 2021)
Key exercises during this phase included isometric rotator cuff activation in safe, non-provocative positions, scapular stabilisation targeting the lower trapezius and serratus anterior, closed-chain stability work, and education about the surgical pathway and what to expect in recovery.

The Rehabilitation Journey
Post-operative rehabilitation was structured in clear phases, each one gated by objective strength and functional milestones — not just the passage of time.
Weeks 6-10: Restore movement, activate the cuff.
Formal post-op physiotherapy commenced at six weeks. We focused on gentle range of motion restoration, isometric rotator cuff activation progressing to light Theraband resistance, and rebuilding scapular control — the foundation everything else sits on.

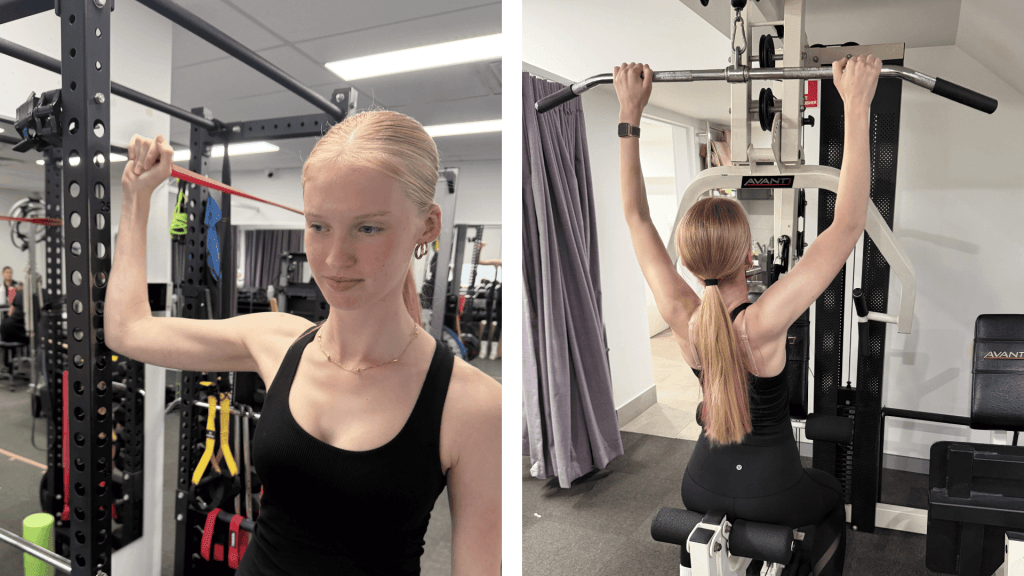
Weeks 10-16: Build strength progressively.
Elise progressed into the gym with seated and bent-over rows, lat pulldowns, banded chin-ups, shoulder press, and heavier resistance band rotator cuff work in more functional ranges. Advanced strengthening was held off until 10 to 12 weeks post-operatively, in line with the biological timeline of labral healing. (Smith et al., 2023; Hanchard et al., 2022)
Weeks 16-21+: Sport-specific and reactive training.
This phase replicated the demands of netball — throwing, landing, overhead loading, and reacting to unexpected forces. We introduced plyometric push-up progressions, Swiss ball and medicine ball work, overhead throws, and perturbation training. Progressive rotator cuff loading with perturbation-based stability work is a cornerstone of post-operative rehabilitation for shoulder instability. (Jaggi et al., 2023)

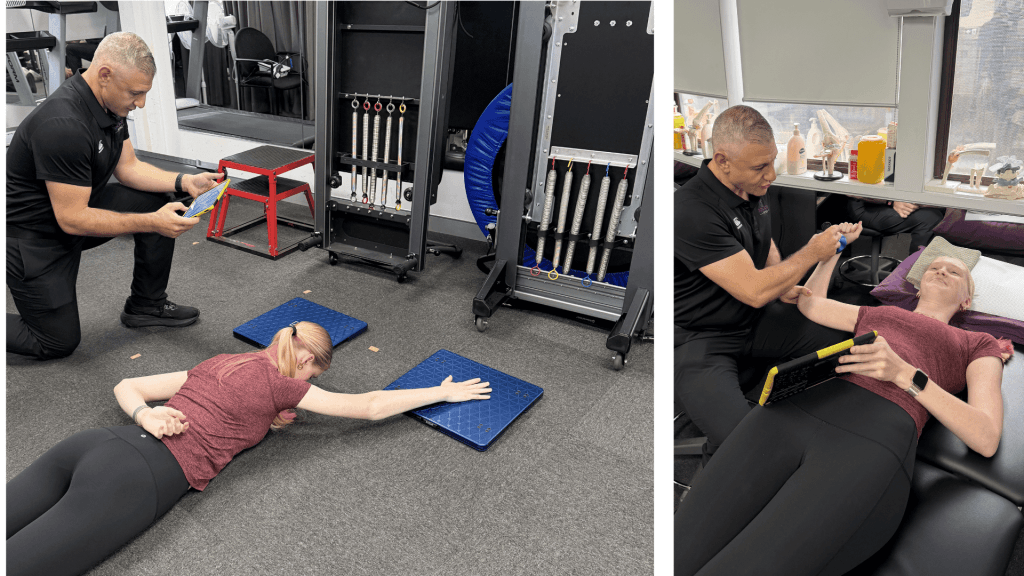
Objective Outcomes: Measuring What Matters
Elise’s strength and function were tracked throughout using AxIT handheld dynamometry and force plates as well as standardised functional tests. Objective measurement provides reproducible data to guide progression and support return-to-sport decisions — moving beyond “how does it feel” to “what does the data show”. (Hickey et al., 2023)
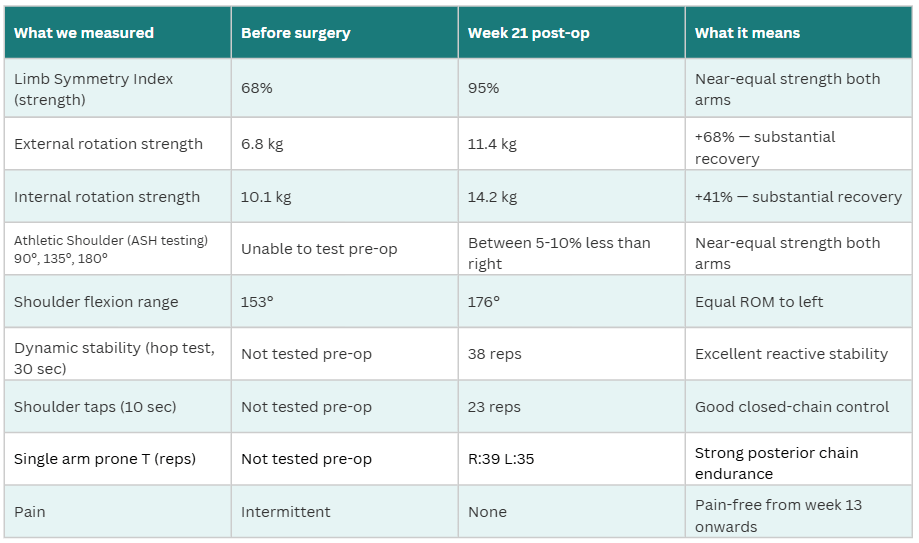
By 21 weeks post-operatively, Elise had achieved near-symmetrical strength, full functional range, and excellent dynamic stability scores. She was pain-free from week 13. Post-operative return-to-sport rates of 80 to 90% are reported in appropriately selected young athletes following arthroscopic stabilisation. (Hurley et al., 2020; Robinson et al., 2022)
We can happily report, Elise is now back to full competition.
Key Takeaways
- Shoulder dislocations in young, active people are not a “shake it off” injury. Each episode causes more structural damage and makes recovery harder — early assessment and specialist review when warranted matter. (Olds et al., 2022; Willemot et al., 2022)
- Physiotherapy can absolutely manage shoulder instability. But when the joint is structurally compromised and the sport is high-demand, surgery is often the evidence-based choice for long-term stability. (Hurley et al., 2020; Longo et al., 2020)
- Pre-operative physiotherapy is not a box-tick — it actively improves post-operative outcomes. (McIsaac et al., 2022) Early referral helps.
- A structured, staged rehabilitation program with objective testing means progression decisions are based on data, not just symptoms. Pain resolution is not a proxy for readiness. (Warby et al., 2020; Hickey et al., 2023)
- Good outcomes like Elise’s are the product of good surgical care, a committed patient, and a rehabilitation program that knows when to push and when to protect.
If you or someone you care for has an injury, a flare up, requires some rehabilitation or experiences an increase in pain, give the clinic a call on 9713 2455 or book online.